
There is an ongoing debate about the role of inert placebos in vaccine clinical trials. What is rarely acknowledged is that many vaccine trials do not, and cannot, use a true inert placebo.
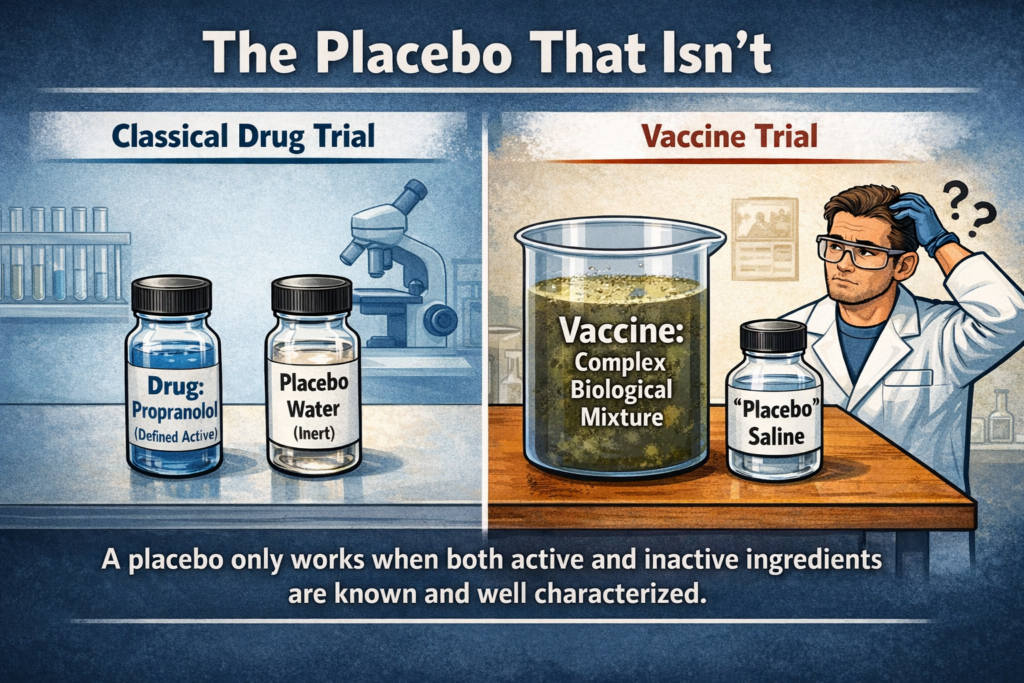
Arguably, the very concept of a placebo originates from classical drug development, where the intervention (drug) typically involves a simple, well-defined active ingredient. Consider, for example, a study evaluating the efficacy of propranolol, a beta-blocker used to lower blood pressure. One group of patients receives a solution containing propranolol dissolved in water, while the control group receives water alone. Neither the patients nor the drug administrators know which treatment has been given (a double-blinded design). Outcomes—such as changes in blood pressure—are measured objectively, and the results are analyzed only after the treatment codes are revealed.
Similarly, for tablet-based drugs, two types of tablets are prepared: one containing the active ingredient and the other containing no active ingredient (a dummy tablet, often composed of inert substances such as sugars or fillers). Both tablets otherwise contain the same inactive excipients and are administered under identical conditions. This approach is scientifically valid because both the tested product and the analytical methods used to measure outcomes are well defined, validated, and grounded in established analytical chemistry.
However, serious problems arise when this classical framework is transferred to virology and vaccine trials. Vaccines are not simple, single-component drugs. They are complex mixtures composed of known and unknown components, often derived from cell cultures with added substances. In practical terms, a vaccine is a heterogeneous “soup” for which no clear qualitative or quantitative characterization, nor validated methods to establish such characterization, are available.
In classical drug trials, the active ingredient is clearly identified, and the remaining ingredients are demonstrated to be inert. In contrast, with vaccines, the entire formulation constitutes the intervention, yet its full composition and behavior are not adequately characterized, at least from a chemical standpoint. As a result, defining a true placebo becomes problematic. A genuine placebo would need to contain everything except the presumed active agent (for example, mRNA in mRNA vaccines).
However, without an isolated or purified sample of that presumed agent, validated methods to identify and quantify it, and independent proof of its existence, there is no reliable way to determine whether it is present or absent. Moreover, unlike classical medicines, vaccines contain additional components—many of them biologically active or insufficiently defined—which further undermines the validity of placebo-based comparisons.
Because the composition of the vaccine cannot be fully determined, the same uncertainty applies to any so-called placebo. Using water or saline as a placebo is therefore scientifically invalid, because such a comparison sets the entire vaccine mixture against an unrelated substance rather than isolating the effect of a defined active component.
As a result, no valid clinical trial can be conducted to evaluate vaccine efficacy in the traditional sense. This is precisely why true placebo-controlled vaccine trials are absent. Instead, this fundamental limitation is often bypassed by claims that alternative methodologies are acceptable, or that prior studies somehow validate newer ones without a placebo. These justifications do not resolve the underlying scientific problem.
An additional, equally problematic practice is comparing new vaccines to previously approved vaccines. This argument is particularly weak: comparing one poorly characterized mixture to another does not establish the efficacy or safety of either. In effect, one undefined preparation is measured against another undefined preparation, yielding no meaningful scientific insight.
In summary, it is not possible at present to conduct proper clinical trials for vaccines using a genuine inert placebo, whether water, saline, or any other substance. Comparing one vaccine to another only compounds the problem. Nevertheless, medical authorities continue to treat such studies as valid clinical trials and to assert efficacy and safety on that basis. From a scientific standpoint, however, no clinically valid trials can be conducted—only the appearance of them.