In principle, efficacy is intended to represent the proportion of patients who are cured. Traditionally, this has been inferred from clinical improvement—the resolution of visible or reported symptoms. More rigorously, however, a true cure should be demonstrated objectively through testing, using measurable markers whose changes reliably reflect disease progression or recovery.
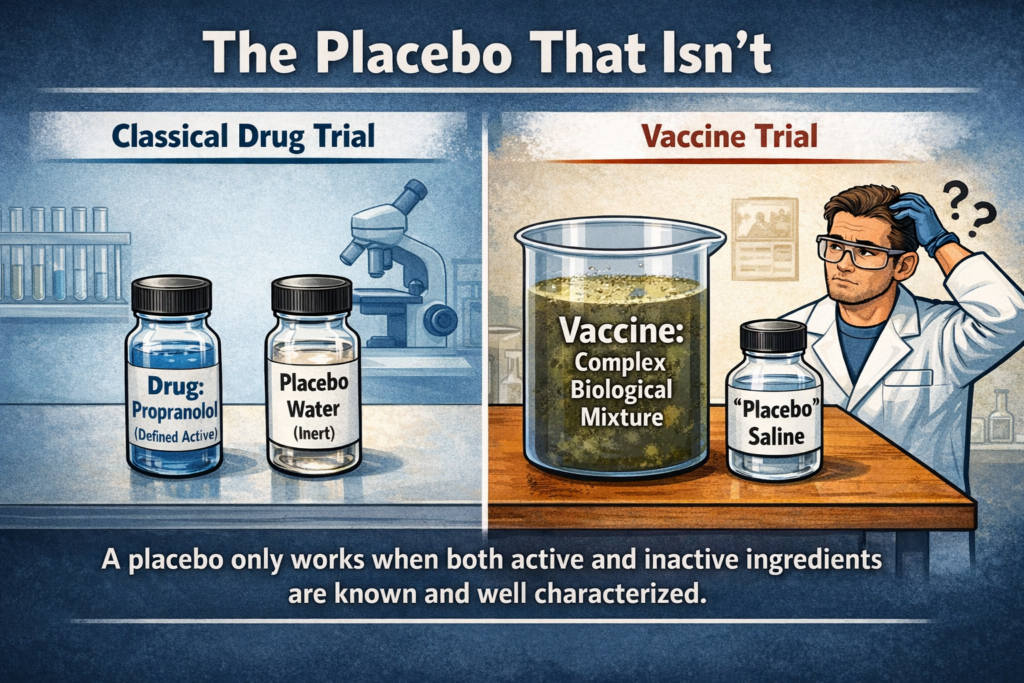
For example, in the case of a viral infection, effective treatment would be expected to reduce viral load or specific viral markers, such as viral RNA or proteins. This framework assumes that such markers are elevated in sick individuals compared to healthy ones, and that their reduction corresponds to recovery. This is the model upon which claims of efficacy are meant to rest.
However, this framework does not operate in virology as practiced today. There is no scientific evidence demonstrating the existence of viruses as claimed, and therefore, no validated evidence for their supposed markers. As a result, the fundamental requirements for objective measurement are neither met nor applied.
(more…)