Read the comment carefully and critically (provided below). It unintentionally exposes the core issue.
What is being acknowledged here is that vaccination is market-driven, not driven by public health necessity or medical urgency. Investment decisions are openly framed in terms of return on investment and market access, not disease burden, scientific need, or demonstrated efficacy.
This immediately raises an obvious question:
What happened to the alleged existential threat of viruses and pandemics?
The referenced policy shift primarily applies to the United States, which represents only a small fraction of the global population. If the claims about viral threats and the necessity of vaccination were scientifically sound, one would expect overwhelming demand, urgency, and justification from the rest of the world. That has not occurred. No global scientific or public-health case has been convincingly made to support continued investment.
This is consistent with what I have been stating all along: viruses have not been scientifically demonstrated as physical entities, and vaccines therefore lack scientific relevance. When funding— which creates the market, not pathogens or their treatment— is withdrawn, development stops not because of politics, but because there is no defensible scientific foundation to sustain it.
I will go further. HHS and other authorities should apply the same level of scrutiny to the diagnosis and treatment of many so-called diseases, including cancer. From a true scientific perspective, many modern diagnoses and treatments lack proper scientific grounding. They are based on assumptions, surrogate markers, and narratives rather than isolated, purified, and characterized causes.
Medical science repeatedly claims scientific authority, yet it does not operate within the framework of true science. It lacks rigorous physical verification, analytical validation, and causal demonstration. As a result, many conditions are likely misdiagnosed and mistreated—potentially representing unresolved microbial processes that could be addressed with appropriate antimicrobial approaches, rather than the current aggressive, often ineffective interventions, but highly expensive (profitable) treatments.
This is not a political argument. It is a scientific one.
When science is real, markets follow necessity. When markets collapse, it is often because the science never existed in the first place.
Text from the referenced article/post.
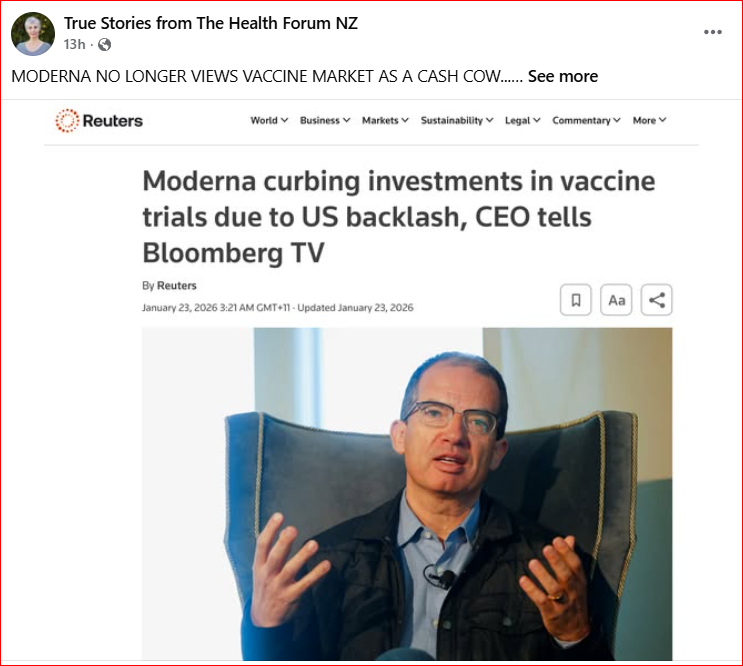
“MODERNA NO LONGER VIEWS VACCINE MARKET AS A CASH COW…
Bloomberg) — Moderna Inc.’s chief executive officer said the company doesn’t plan to invest in new late-stage vaccine trials because of growing opposition to immunizations from US officials.
“You cannot make a return on investment if you don’t have access to the US market,” Stéphane Bancel said in an interview with Bloomberg TV from the World Economic Forum in Davos, Switzerland. Regulatory delays and lack of support from US health officials are making the potential market size “much smaller,” he said.
Bancel’s comments are some of his strongest yet about the difficulties that vaccine makers face in the Trump administration. He joins a chorus of other pharmaceutical executives who have started to vent their frustrations with the government’s assault on immunizations.
“It’s sad for us to see that vaccines that have been proven for decades helping people around the world are not recommended anymore,”