The vaccine debate is commonly presented as a clash between science and skepticism. In reality, it is a dispute between competing authorities—neither of which is grounded in the standards of true science.
The Illusion of Scientific Authority in Modern Medicine
From a scientific perspective, the public is largely unaware of a crucial fact: neither side of the contemporary vaccine debate is grounded in true scientific expertise.
In the case of Robert F. Kennedy Jr., this limitation is openly acknowledged. He does not claim training in chemistry, physics, or analytical science. That point is neither disputed nor concealed.
What is far less recognized—and far more consequential—is that the same limitation applies to Anthony Fauci, as well as many other high-profile physicians routinely portrayed as “science experts.” Despite their medical authority, they do not possess academic training or credentials in true science—namely, chemistry, physics, or analytical measurements. Yet their work is repeatedly labeled “science,” often under the terms medical science or virology.
This distinction is not semantic. It is foundational.
Medical Authority Is Not Scientific Authority
Medicine is a practice-based profession. It applies tools and products developed elsewhere. Drugs are chemicals. Diagnostics are measurements. These domains belong to chemistry and analytical science, not to medicine itself.
Modern medicine, however, has adopted scientific language without adhering to scientific standards. Claims involving viral isolation, PCR testing, immune markers, and vaccine efficacy are presented as established science, despite lacking the foundational requirements of true scientific disciplines.
As a result, opinions from both political critics and medical authorities lack scientific credibility when examined against the standards of chemistry and analytical chemistry.
Asking Questions Does Not Require Scientific Credentials
This is where the debate must be reframed.
A consumer does not need to be a mechanical engineer to evaluate a car. One is not asking how an engine works or to redesign it; one asks for evidence of performance. Does it meet specifications? Does it perform as claimed? Is there verifiable data?
The same logic applies here.
RFK Jr. does not need to be a chemist or scientist to ask simple, legitimate questions:
- Where is the physical sample of the virus to verify the claim of its existence?
- Where is the study protocol demonstrating vaccine efficacy against viruses or their diseases?
- Where are the measurements calibrated against known standards (viruses, RNA, mRNA, spike protein, etc.?
These are not political questions; they are basic scientific questions—or the same questions any informed consumer would reasonably ask.
Where the System Fails
When such questions are raised, the response from medical authorities is predictable:
“The science is settled.”
“The data are peer-reviewed.”
“There is consensus.”
This is precisely where the failure becomes visible.
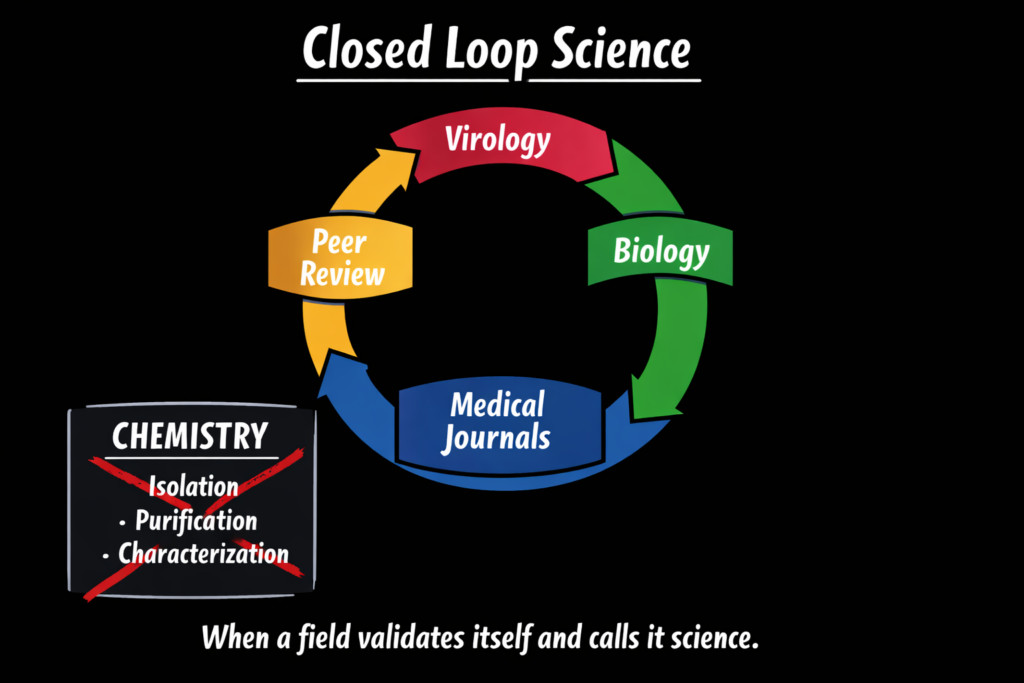
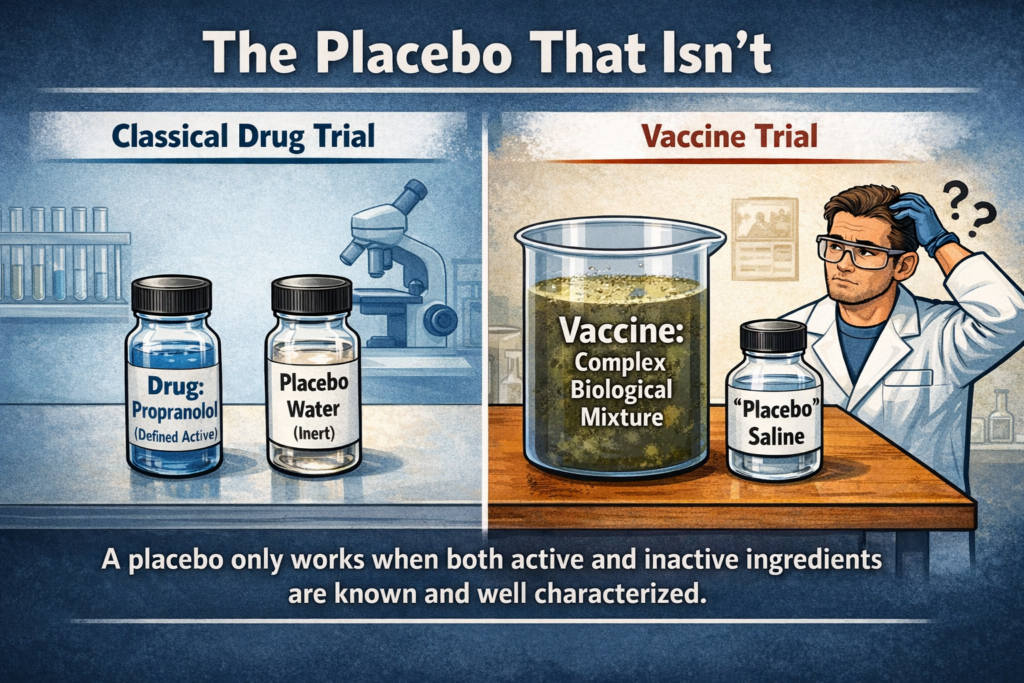
Peer review in medicine is internal—conducted by similarly trained practitioners—not external validation by scientists trained in chemistry or analytical measurement. PCR testing, which underpins modern virology, has never been scientifically validated against a pure, isolated, and characterized physical virus sample—because such a sample has never been produced.
Without a physical reference, no test can be scientifically validated. Without validated tests, no illness can be scientifically attributed. Without that attribution, efficacy cannot be established—only assumed.
Why RFK Jr. Needs True Science Support
This is not a political weakness. It is a structural one.
RFK Jr. can ask the right questions, but without support from true science experts—particularly analytical chemists—those questions are easily deflected by appeals to authority. That is how fake science survives: not by evidence, but by insulation.
A single sentence from an analytical scientist exposes the entire framework:
Without a pure, isolated physical virus sample, none of the claimed tests, diagnoses, treatments, or vaccines can be scientifically validated.
Nothing more is required.
The Consequences of Facing Reality
Once this issue is examined through the lens of true science, the implications are unavoidable.
If viruses have not been scientifically demonstrated through isolation, purification, and characterization, then illnesses attributed to them cannot be scientifically established. If those illnesses are not established, then claims of treatment efficacy—including vaccines—have no scientific foundation. Without a verified target, there can be no validated test, no calibrated measurement, and no meaningful assessment of efficacy.
What follows is not a minor correction but a systemic collapse. Testing protocols, efficacy claims, regulatory approvals, and public-health mandates all rest on assumptions that have never been validated by the standards of chemistry or analytical science. Remove those assumptions, and the entire structure fails simultaneously.
This is not a matter of opinion. It is a matter of scientific necessity.
A Clear and Shorter Path Forward
Because the problem is foundational, the resolution does not require endless debate, more funding, or decades of additional research. It requires only one thing: the application of real science.
If chemistry and analytical science were applied honestly, the discussion would conclude quickly. Either a physical virus sample exists and can be produced for independent validation—or it does not. Either diagnostic tests can be calibrated against that physical reference—or they cannot. Either efficacy can be demonstrated against a verified illness—or it cannot.
There is no middle ground.
This is why the issue persists. Not because the science is complex, but because it has never been properly applied. The system survives by avoiding the very standards it claims to uphold.
Once those standards are enforced, the debate ends—not slowly, but immediately. And with it ends the illusion of “medical science” as a substitute for real science.
Conclusion
This debate persists only because true scientific standards have been excluded from the discussion. Once chemistry and analytical science are applied, the foundations of modern virology and vaccination collapse under their own weight. What remains is not science, but belief reinforced by authority and repetition. Real science does not require consensus, peer approval, or institutional protection—it requires evidence. And that evidence has never been produced.