Learning and managing science or scientific research by doctors (medical science experts) is like learning from a pitstop tech about the oil industry (exploration, extraction, processing, etc.) who claims to have seen it all in the world of oils and lube in the shop (“clinics”).
Interestingly, the pitstop tech may be better qualified as they can show samples of lube and oils, not the medical experts who cannot show what they have been working with.
I am serious!
Medical experts (physicians) are educated and trained to write prescriptions using some technical vocabulary (most from science/chemistry). They have no education or understanding of the actual science or scientific (lab) research.
The public and their leadership must consider this fact, particularly at CDC/FDA/HHS. Years of work (“research”) with billions of dollars of funding for virus works, but no samples of viruses to show. What do these “scientists/researchers” work with or on?
mRNA Vaccine Is Not mRNA But Gunk – A Forensic Analysis (link)
Cancer and Ivermectin (link)
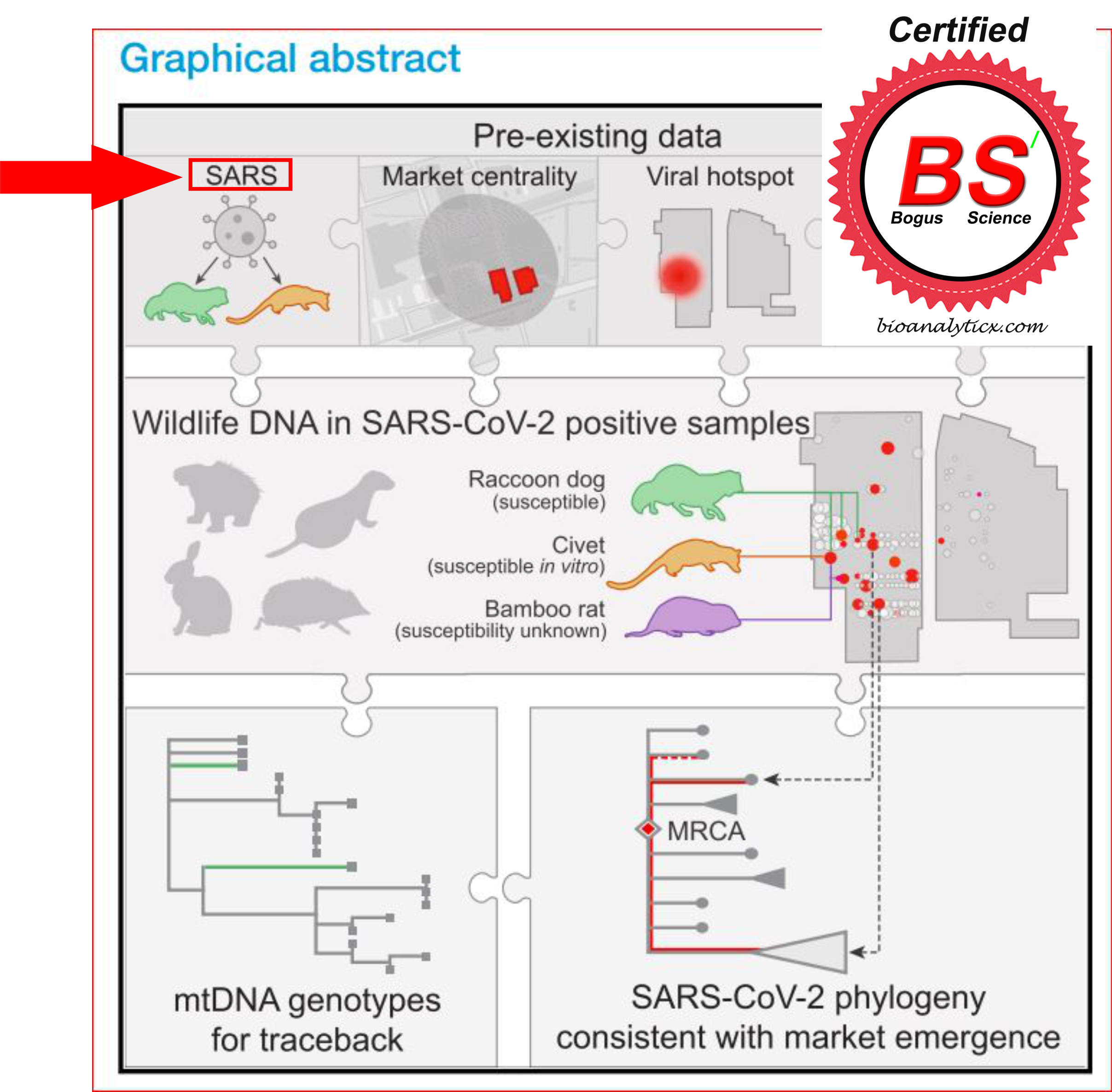
COVID-19: The virus does not exist – it is confirmed! (link)
Who Is Corrupt: Doctors Or Pharma? Check It Yourself (link)
Vaccines: Useless But Dangerous Soup/Gunk That Must Be Purged (link)
Vaccine Science: Nonsense And BS! (link)
An M.D. degree is not a science degree! (link)
What is science, and who are scientists? link
My training and expertise – people ask! link